How three researchers achieved scientific distinction with single cell and spatial technologies

Whether it’s treating cancer, understanding Alzheimer’s disease, or bringing down costs, every scientist shares a common aim: to make an impact. Oftentimes, that impact is achieved by taking novel ideas and marrying them to new tools that make it possible.
In this article, we’re highlighting three researchers who’ve already made major impacts—and are just getting started making more. We bring together several interviews with them to showcase their work, how single cell and/or spatial technologies made their research possible, and where they see these cutting-edge tools taking them. Allow us to introduce:
- Sneha Ramakrishna, MD (Stanford University): Moving the needle on pediatric glioma therapies
- Nick Banovich, PhD (The Translational Genomics Research Institute (TGen), part of City of Hope): Understanding pulmonary fibrosis and drastically reducing per-sample spatial transcriptomics costs
- Alon Millet (Graduate Student Researcher, Rockefeller University): Identifying a novel cell type associated with Alzheimer’s disease
Dr. Ramakrishna
Can you tell us a little about your work?
The project that we're discussing is in the context of a GD2 CAR T-cell trial for treating pediatric patients with diffuse midline glioma, which is a universally fatal tumor. There are no curative options for these patients and, unfortunately, the median overall survival time is about 11 months.
Not only are there no treatment options, but it's really very difficult to control this tumor even for a short period of time. The only treatment that these patients get is radiation therapy and following that, there's no other treatment option available for these patients.
Thanks to the generosity of patients who have donated their brain tissue after they’ve passed, we’ve been able to learn more about the biology of these tumors. In a collaboration between Drs. Michelle Monje and Crystal Mackall, led by Drs. Chris Mount and Robbie Majzner, our team at Stanford identified that GD2 was highly and uniformly expressed in diffuse midline glioma tissues. We showed we could target these tumor cells using GD2 CAR T cells in mice. And we were able to open a clinical trial and bring this to patients.
What made you choose single cell and/or spatial transcriptomics for your research? How have they helped?
I came into the study basically saying, okay, how do we learn from our patients? How do we really understand the immune biology of what will make these CAR T cells work—or not—for our patients?
So we collected patient cerebrospinal fluid (CSF) samples at specific time points throughout the treatment course. We realized, however, that people weren't capturing the cellular population when they tried to do flow, both because of the limited cell counts from CSF and because freezing the samples reduces viable recovery.
We took the sample straight from the bedside to the bench and processed it fresh on the Chromium single cell RNA-seq platform. This allowed us to capture the cellular populations consistently over the course of the treatment, and it gave us insight into what immune populations contributed to whether the CAR T cell worked in our patients.
From this robust dataset, we saw that the predominating populations are myeloid and T cells. They fluctuate over the treatment course, and we’re working on figuring out the specific immune populations that contribute to patient response versus when they stop responding and patients start to progress.
When we got CSF samples, the question was whether they’re representative of what's happening in the brain and the tumor. Spatial transcriptomics is really one of the most sensitive ways to delve deep into that question, and we were looking for the same immune populations in the tumor tissue, so we collaborated with our 10x Genomics colleagues to create a custom Xenium panel based on our CSF findings.
In our initial validation of this panel, we've been able to consistently see our CAR T cells. That’s wonderful because it lets us see if there are CAR T cells in the tumor tissue at the time of collection, and it also lets us define the different immune populations at a single cell level.
[...]If we're going to learn from the patients, we have to learn everything we can from all the tissue we get. This is the best way that I can think of to honor these brave patients.
What does the future hold?
In pediatric oncology, if you're not curing a patient you're not doing enough. We will never settle for less than a cure. But this trial finally moved the needle. We finally made a difference in a disease that we’ve literally never made a difference in before.
In fact, in our paper, we have a patient who was a complete responder: not only did the tumor go away, it hasn’t recurred for over three years. This is a patient who, when we met them, they weren't sure if they were going to graduate from high school. Now they're in college and living their best life. They actually gave an interview recently.
This is the dream of something that we could do for a single person. And hopefully, by taking what we learn from this individual, it becomes something we can do for all of them. That’s the power of incorporating these assays into our studies, because we can use the knowledge they give us to keep pushing that needle forward. And we won’t stop until we reach that goal.
[Back to top]Dr. Banovich
Can you tell us a little about your work?
One of my roles at TGen is to operate our spatial transcriptomics technology core. The core offers Xenium and Visium HD as services to both internal investigators at TGen as well as external investigators outside of our institute.
My primary function is my research lab, which is focused on understanding how gene regulatory changes impact disease outcomes. Over the past several years, we've built our foundation on single cell transcriptomics and using this to understand the molecular dysregulation of disease with cell-type resolution.
One of our major projects is focused on pulmonary fibrosis. We also focus on correlative analyses from patients undergoing CAR T-cell therapies for brain tumors. So we use very different biological systems, but they’re unified by the set of tools and approaches, i.e., looking at molecular dysregulation in disease at cell-type resolution.
What made you choose single cell and/or spatial transcriptomics for your research? How have they helped?
Over the past couple of years, we've started to put more of a focus on spatial technologies, and we've been using the Xenium platform since February of 2023. We think about the same types of concepts that we thought about in single cell, but obviously spatial data has a lot of benefits: understanding not just the cell-type-level dysregulation, but the organization of cells into architectural niches.
One of the things that's unique about Xenium, and unique about imaging-based spatial transcriptomics, is that it's the first time in genomics, since the advent of next generation sequencing, where we're not doing an assay and then putting that on a sequencer. It's really an all-in-one platform.
Because of that, our cost drops linearly as we add more samples to a single run. We were early adopters of single cell multiplexing approaches. Those drop the front-end cost, but the sequencing costs increase with greater numbers of cells. With Xenium, it costs the same to analyze 10% of the available sample area as it does to analyze 100% of the available tissue area, so there’s a true linear cost drop.
What does the future hold?
The anecdote I like to use is that the oldest sample we've profiled was about 15 years old. It had just sat on my collaborator’s desk in a shoebox that he touched and dug through with bare hands over the course of those years—everything that just makes us, as RNA people, die on the inside, you know? Except we were still able to get good data from it. So I think Xenium has the ability to perform on those kinds of archival tissue samples.
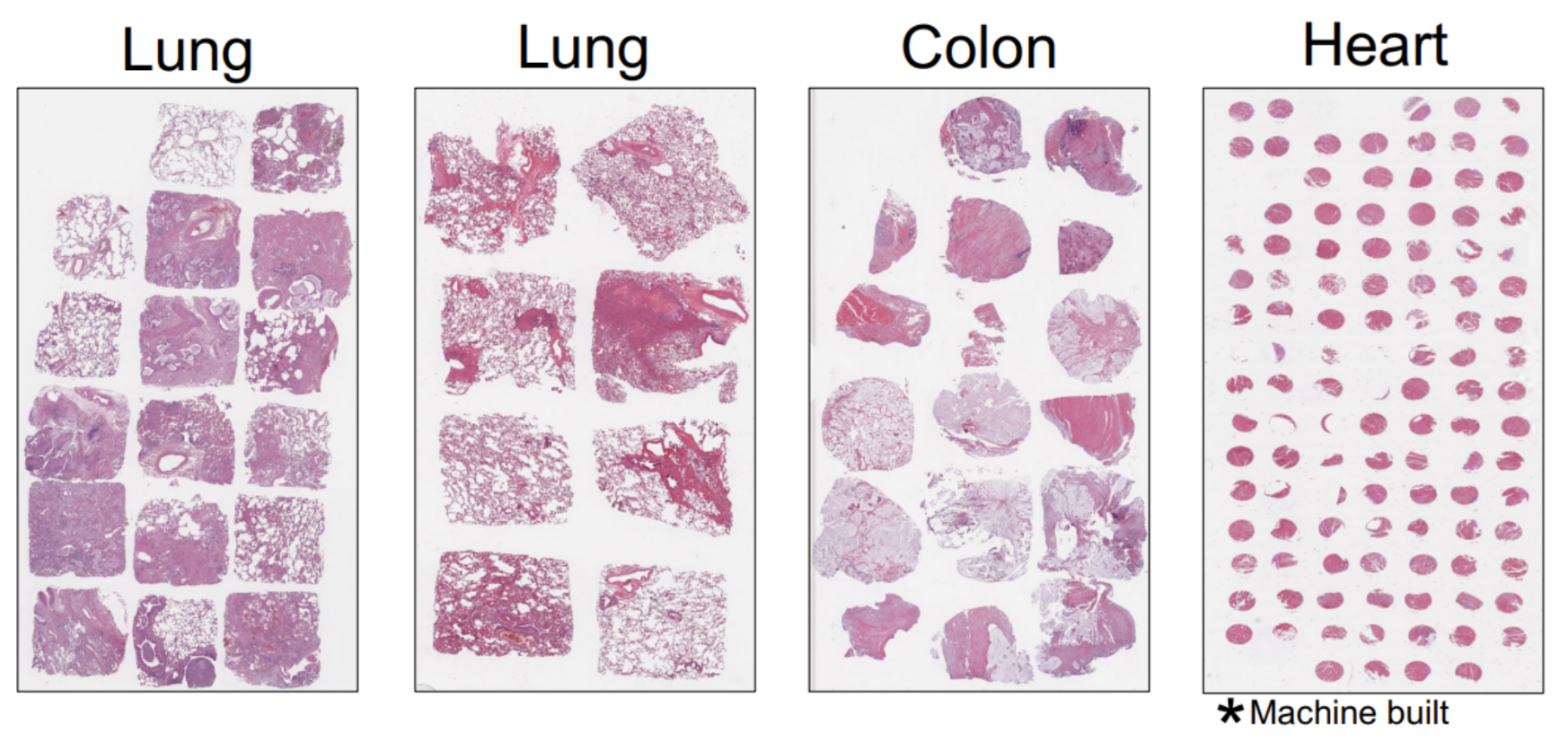
This catapults us into the next part of our conversation—the ability to use FFPE samples in these tissue microarray approaches (Figure 1) is part of what really made us excited about the Xenium platform. The combination of the FFPE compatibility, as well as the high throughput of the Xenium system, helps us start to envision how we might really do these projects at scale.
What I mean is, instead of just ten or fifteen samples, we can start thinking about hundreds of samples that we could process.
[Back to top]Alon Millet
Can you tell us a little about your work?
A major risk factor for Alzheimer’s disease is APOE4, and I identified a new microglial state that's strongly enriched in APOE4 carriers and becomes more enriched with age and disease progression. I showed that these microglia probably contribute to disease by being unable to clear amyloid beta and participating in inflammatory crosstalk with other immune cells. I also showed that currently existing therapeutics for Alzheimer's disease, such as aducanumab, clear this cell state back to a more functionalized role.
The second part of my work is still in progress. It uses single cell biology looking at physiological immunity in completely healthy mice and healthy individuals, and asks how common APOE mutants impact fitness and the state of the immune system. That work has led to some very interesting questions that are starting to turn mechanistic.
The common thread between these, though, was leveraging computational biology and using big single cell datasets to identify interesting phenotypes that can then be really explored at a more basic level.
What made you choose single cell and/or spatial transcriptomics for your research? How have they helped?
The first tool we used in the paper was single cell sequencing with Chromium Universal 3’ Gene Expression to see if there were changes in heterogeneity in APOE2, -3, and -4 microglia over the course of Alzheimer's disease progression.
The next tool that we used was multiome single cell sequencing with Epi Multiome ATAC + Gene Expression to identify not just the transcriptional state and how it varies in this model, but also what happens to the epigenome. This approach was critical for us to identify molecular features and drivers that produce this state in the first place.
Having both single cell ATAC- and RNA-seq data from the same cells let us build some really nice computational models of the gene regulatory networks that undergird each of these different microglial states, and that lets us identify putative transcription factors that influence their state.
Spatial was a natural extension of that. We’d found the cell state, now we wanted to know what it’s up to, what it’s surrounded by, and use that to figure out phenotypic outputs. Spatial tipped us off to the fact there are differences in their surroundings with respect to amyloid beta.
We were able to look at the niche around these cells and find that they're surrounded by astrocytes that overexpress amyloid precursor protein (APP). So you see that one of these stressed microglia is literally always right next door to one of these astrocytes that overexpress APP.
This kind of analysis is only possible through spatial, and it led us naturally to these next steps of a potential disease mechanism.
What does the future hold?
Following up on the Alzheimer's story, there are two questions I’m really interested in. The first is to what extent the microglial subtype I identified is also relevant to non-Alzheimer’s disease neuroinflammation, such as multiple sclerosis, brain tumors, etc.
Question number two is whether, and to what extent, these cells are a therapeutic target. If we had some way to reliably revert these cells back to a more functionalized state, could that be therapeutic?
Finally, we’re interested in how targeting APOE might impact the emergence of these cells. There’s a company associated with our lab, and one of their products is an APOE agonist. We’re curious about what happens if we give this drug to Alzheimer’s model mice, to see if it has any impact on disease progression.
I also alluded to my interest in clinical trials and translational findings. I think spatial offers the opportunity to do more and better drug testing, better drug screening—getting a better idea of what’s going on in the brain.
[Back to top]These researchers have already made impacts and left their mark on cancer, Alzheimer’s disease, lung disease, and more by using single cell and spatial technologies. The only question is, what will your impacts be? See what’s possible with single cell and spatial transcriptomics technologies and find out.
These interviews have been edited for length and clarity. We'd like to thank these three scientists for their contributions to this blog!


